
Congenital hyperinsulinism is characterized by inappropriate and unregulated insulin secretion from the beta-cells of the pancreas. In CHI the beta-cells release insulin inappropriately all the time and insulin secretion is not regulated by the blood glucose level (as occurs normally). The action of insulin causes hyperinsulinaemic hypoglycaemia. High insulin levels prevent ketone bodies being made. This means that the brain is not only deprived of its most important fuel (glucose), but also ketone bodies which are used as alternative fuels. Repeated episodes of low blood sugar and high insulin levels increase the risk for serious complications such as breathing difficulties, seizures, intellectual disability, vision loss, brain damage, and coma.
What is a normal blood glucose level in CHI?
For the purpose of CHI, hypoglycaemia is agreed to be less than 3.5mmol/litre. In the absence of ketone bodies, infants with CHI are constantly reliant on the circulating blood glucose as the fuel for normal neurological functioning, hence the importance of maintaining the blood glucose concentration above 3.5mmol/litre.
Watch this video from The University of Manchester to learn more about the effects of Hypoglycaemia in Congenital Hyperinsulinism (CHI)
What causes CHI?
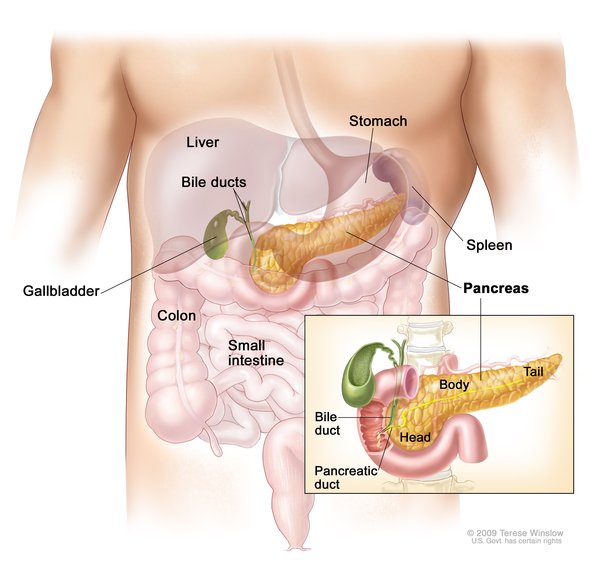
Congenital hyperinsulinism (CHI) is caused by mutations in genes that regulate the release (secretion) of insulin, which is produced by beta cells in the pancreas. Insulin clears excess sugar (in the form of glucose) from the bloodstream by passing glucose into cells to be used as energy.
Gene mutations that cause congenital hyperinsulinism lead to over-secretion of insulin from beta cells. Normally, insulin is secreted in response to the amount of glucose in the bloodstream: when glucose levels rise, so does insulin secretion. However, in people with congenital hyperinsulinism, insulin is secreted from beta cells regardless of the amount of glucose present in the blood. This excessive secretion of insulin results in glucose being rapidly removed from the bloodstream and passed into tissues such as muscle, liver, and fat. A lack of glucose in the blood results in frequent states of hypoglycemia in people with congenital hyperinsulinism. Insufficient blood glucose also deprives the brain of its primary source of fuel.
Mutations in at least nine genes have been found to cause congenital hyperinsulinism. Mutations in the ABCC8 gene are the most common known cause of the disorder. They account for this condition in approximately 40 percent of affected individuals. Less frequently, mutations in the KCNJ11 gene have been found in people with congenital hyperinsulinism. Mutations in each of the other genes associated with this condition account for only a small percentage of cases. In approximately half of people with congenital hyperinsulinism, the cause is unknown.
Inheritance patterns in CHI
Congenital hyperinsulinism can have different inheritance patterns, usually depending on the form of the condition. At least two forms of the condition have been identified. The most common form is the diffuse form, which occurs when all of the beta cells in the pancreas secrete too much insulin. The focal form of congenital hyperinsulinism occurs when only some of the beta cells over-secrete insulin.
Most often, the diffuse form of congenital hyperinsulinism is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
Less frequently, the diffuse form is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder.
The inheritance of the focal form of congenital hyperinsulinism is more complex. For most genes, both copies are turned on (active) in all cells, but for a small subset of genes, one of the two copies is turned off (inactive). Most people with the focal form of this condition inherit one copy of the mutated, inactive gene from their unaffected father. During embryonic development, a mutation occurs in the other, active copy of the gene. This second mutation is found within only some cells in the pancreas. As a result, some pancreatic beta cells have abnormal insulin secretion, while other beta cells function normally.
Watch this video from The University of Manchester to learn more about the genetics and diffuse Congenital Hyperinsulinism (CHI)
In this video, also from the University of Manchester, you can learn more about focal Congenital Hyperinsulinism (CHI)
How common is CHI and whom does it affect?
Hypoglycaemia, due to CHI, is a relatively rare but potentially serious condition occurring soon after birth. The estimated incidence of CHI is one in every 40,000 to 50,000. It is much more common in communities where marriage between blood relatives occurs, possibly as frequently as one in every 2500 children.
Other names for congenital hyperinsulinism (CHI): Hyperinsulinemia hypoglycemia of infancy, infancy hyperinsulinemia hypoglycemia, neonatal hyperinsulinism, persistent hyperinsulinemia hypoglycemia of infancy, persistent hyperinsulinemic hypoglycemia, PHHI hypoglycemia, CHI, Hyperinsulinisme.